If you’ve noticed a bulge in your groin, belly button, or abdomen—or felt a persistent ache that worsens when you cough, lift, or stand—you’re likely searching for one urgent answer: Can a hernia heal itself?
The short, evidence-based answer is no for the vast majority of adult hernias. A hernia is a permanent structural defect in the abdominal wall or diaphragm. Unlike a muscle strain or minor tear that can scar over and strengthen, the opening does not close spontaneously in adults. However, not every hernia demands immediate surgery. Some small, asymptomatic ones can safely be monitored through “watchful waiting,” and certain pediatric cases (especially umbilical hernias in babies) often resolve naturally.
This comprehensive guide—drawing from authoritative sources like the Cleveland Clinic, Mayo Clinic, NHS, and long-term clinical trials—covers everything you need to know. You’ll learn the medical reality, type-specific insights, when monitoring is appropriate, lifestyle strategies to prevent worsening, surgical options, recovery timelines, and red-flag symptoms requiring emergency care. By the end, you’ll have the clarity to discuss options confidently with your doctor.
Important Disclaimer: This article is for educational purposes only and is not a substitute for professional medical advice. Hernia evaluation requires a qualified healthcare provider. Always seek personalized diagnosis and treatment.
What Is a Hernia? Understanding the Structural Defect
A hernia occurs when an internal organ or tissue (usually intestine or fat) pushes through a weakened spot in the surrounding muscle or connective tissue. Think of it like a tear in a strong canvas: once the fibers separate, pressure from inside the abdomen forces contents outward, creating a visible or palpable bulge.
Hernias develop gradually from cumulative wear-and-tear or suddenly from heavy strain. The abdominal wall is designed to withstand pressure, but factors like aging, obesity, or prior surgery create vulnerabilities. Unlike bruises or sprains, the defect is mechanical—your body cannot “weave” the muscle fibers back together without surgical reinforcement.
Key Fact: Hernias do not heal spontaneously in adults because the hole or weakness persists. Tissue may temporarily reduce (slip back inside), but the underlying defect remains.
Common Types of Hernias and Their Healing Potential
Hernia type directly influences symptoms, risks, and whether natural resolution is even possible.
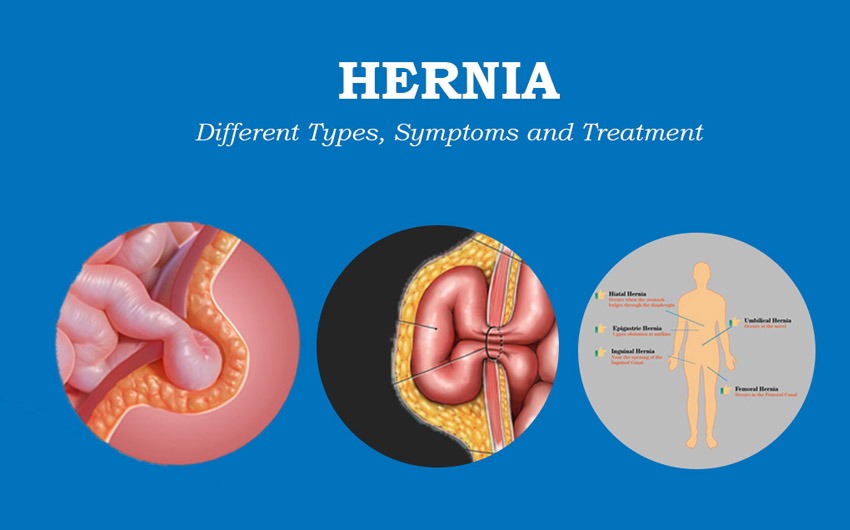
- Inguinal Hernia (75% of all cases, mostly men): Occurs in the groin where the spermatic cord or round ligament passes through the abdominal wall. A loop of intestine or fat protrudes into the inguinal canal.
- Healing potential: Does not heal itself. Watchful waiting is often safe for minimally symptomatic cases in men.

- Femoral Hernia (more common in women): Below the inguinal ligament in the upper thigh. Higher risk of strangulation due to narrow canal.
- Healing potential: No self-resolution; surgery usually recommended sooner.
- Umbilical Hernia: At the belly button. Common in infants (congenital) and adults (from pregnancy, obesity, or fluid buildup).
- Healing potential: Yes in babies—over 90% close by age 5 as abdominal muscles strengthen. In adults: No.
- Hiatal Hernia: Stomach pushes through the diaphragm into the chest. Often linked to GERD.
- Healing potential: Does not heal structurally, but symptoms (heartburn) can be managed medically without surgery in mild cases.

- Incisional Hernia: Develops at the site of a previous abdominal surgery scar.
- Healing potential: No; often requires mesh repair due to weakened tissue.
- Epigastric / Ventral Hernia: In the midline above or around the belly button.
- Healing potential: No self-healing.
- Other (Sports Hernia / Athletic Pubalgia): Not a true hernia but a tear in groin muscles/tendons from repetitive twisting. Can improve with rest and physical therapy.
Takeaway by Type: Only congenital umbilical hernias in young children have a high chance of spontaneous closure. All adult hernias require intervention if symptomatic or enlarging.
Can a Hernia Heal Itself? The Evidence-Based Reality
No—adult hernias cannot heal without intervention.
Reputable medical institutions are unanimous:
- Cleveland Clinic: “With the exception of umbilical hernias in babies, they don’t go away on their own.”
- Mayo Clinic and NHS: Hernias will not get better without surgery in most cases, though some may remain stable.
- Multiple hernia specialists: The defect is a mechanical hole; surrounding tissue cannot regenerate to seal it.
The One Exception — Umbilical hernias in infants: The abdominal wall continues developing after birth. Most close naturally by age 2–5. Larger ones (>1.5–2 cm) or those persisting past age 5 often need repair.
Why the Myth Persists: Reducible hernias can be pushed back in, temporarily relieving the bulge. People mistake this for “healing.” In reality, the weakness remains and usually enlarges over time due to ongoing intra-abdominal pressure.
Watchful Waiting: When Monitoring Is Safe (and When It’s Not)
For minimally symptomatic or asymptomatic inguinal hernias in men, watchful waiting is a well-studied, evidence-based option.
Key clinical evidence:
- 2006 JAMA randomized trial: Watchful waiting was safe; only 23% crossed over to surgery at 2 years, with very low emergency rates (0.3% acute incarceration in first 2 years).
- 12-year Lancet follow-up (2023): About two-thirds eventually opted for surgery, mainly due to increasing pain, but emergency complications remained rare (~1–2 per 1,000 patient-years).
Ideal candidates for watchful waiting:
- Small hernia, easily reducible
- No or minimal pain/discomfort
- No impact on daily activities
- Good surgical risk profile (or high surgical risk due to other conditions)
Not suitable if:
- Pain limits activities
- Hernia is growing rapidly
- Femoral, incisional, or symptomatic hiatal type
- Signs of incarceration (see complications below)
Practical Monitoring Plan:
- Annual (or more frequent) physician visits
- Self-check monthly for size changes or new pain
- Immediate ER visit for sudden severe pain, vomiting, or irreducible bulge
Symptoms: What to Watch For
Common signs include:
- Visible or palpable bulge (may disappear when lying down)
- Aching, burning, or pressure at the site
- Discomfort worsened by standing, lifting, coughing, or straining
- Heavy or dragging sensation
- In hiatal: Heartburn, regurgitation, chest pain
Red-Flag Emergency Symptoms (seek ER care immediately):
- Sudden intense pain
- Bulge becomes firm, tender, red, or purple
- Nausea/vomiting
- Inability to pass gas or have a bowel movement
- Fever
These indicate incarceration or strangulation—tissue blood supply is cut off, risking bowel death within hours.
Causes and Risk Factors
Primary cause: Weakness in the abdominal wall combined with increased pressure.
- Congenital: Present from birth (e.g., patent processus vaginalis in inguinal)
- Acquired: Aging collagen loss, previous surgery, pregnancy, chronic straining
Major risk factors:
- Obesity (increases abdominal pressure)
- Pregnancy (multiple or large babies)
- Chronic cough (smoking, COPD, allergies)
- Constipation or straining during bowel movements
- Heavy lifting or repetitive straining occupations
- Prior abdominal surgery
- Family history or connective tissue disorders
- Advanced age, male sex (for inguinal)
Potential Complications of Untreated Hernias
While many hernias remain stable for years, risks rise over time:
- Incarceration: Contents trapped—painful but not yet life-threatening
- Strangulation: Blood supply cut off → tissue necrosis (requires emergency surgery)
- Bowel obstruction
- Chronic pain or reduced quality of life
Emergency surgery for strangulation carries higher risks (infection, longer recovery) than elective repair.
Diagnosis: How Doctors Confirm a Hernia
- Physical exam: Gold standard—doctor feels the bulge while you cough or strain.
- Imaging (if unclear): Ultrasound (first-line, no radiation), CT scan, or MRI.
- For hiatal: Endoscopy or barium swallow.
No blood test diagnoses a hernia.
Non-Surgical Management: Lifestyle Strategies to Prevent Worsening
While these cannot heal the defect, they reduce pressure and symptoms:
Diet and Weight Management
- Aim for healthy BMI (<25 ideal)
- High-fiber diet (25–30g/day) to prevent constipation: fruits, vegetables, whole grains, plenty of water
- For hiatal hernia: Small frequent meals, avoid lying down after eating, elevate head of bed, limit triggers (spicy/fatty foods, caffeine, alcohol)
Exercise Guidelines
- Safe: Walking, swimming, core-strengthening under guidance (planks, bird-dog with proper form)
- Avoid: Heavy lifting, crunches, exercises increasing intra-abdominal pressure until cleared by doctor
Other Supports
- Hernia truss/belt: May provide temporary symptom relief but does not heal or prevent progression. Use only under medical advice—poor fit can worsen issues.
- Quit smoking: Improves tissue healing and reduces cough.
- Manage chronic cough or constipation promptly.
Hernia Surgery: Modern Options and What to Expect
Surgery (herniorrhaphy or hernioplasty) is the only curative treatment—pushes tissue back and reinforces the wall, usually with synthetic mesh.
Types of Repair:
- Open Repair: Traditional incision; excellent for large or complex cases.
- Laparoscopic: 3–4 small incisions, camera-guided; less pain, faster return to work.
- Robotic: Enhanced precision version of laparoscopic; ideal for bilateral or recurrent hernias.
Mesh is used in >90% of adult repairs and dramatically lowers recurrence (from ~10–15% without mesh to <5%).
Success Rates: 90–98% long-term success in elective cases. Recurrence possible if risk factors persist.
Recovery Timeline (varies by type and patient):
- Same-day or next-day discharge for most
- Light activity: 1–2 weeks
- No heavy lifting: 4–6 weeks
- Full return to work/sports: 2–6 weeks (laparoscopic often faster)
Pain is managed with meds; most patients report significant quality-of-life improvement.
Prevention: Reducing Your Risk or Slowing Progression
- Maintain healthy weight
- Use proper lifting technique (bend knees, not waist)
- Treat chronic cough/constipation
- Strengthen core gradually (after medical clearance)
- Avoid smoking
- For women planning pregnancy: Discuss with doctor if you have known weakness
Living with a Hernia: Practical Expert Tips
Many patients live comfortably for years with monitoring. Track symptoms in a journal. Choose supportive underwear or clothing. Stay active within limits—sedentary life can worsen muscle weakness. Join support communities or ask your surgeon about local hernia centers for specialized care.
Debunking Common Hernia Myths
- Myth: “Rest and time will heal it.” → False; the defect is structural.
- Myth: “A hernia belt will cure it.” → False; temporary support only.
- Myth: “All hernias need emergency surgery.” → False; most are elective.
- Myth: “Exercise can push it back permanently.” → False; may help symptoms but not close the hole.
Frequently Asked Questions (FAQs)
Can a small hernia go away on its own?
No, small adult hernias do not heal spontaneously, though some remain stable for years with watchful waiting.
How long can I safely wait before hernia surgery?
It depends on symptoms and type. Minimally symptomatic inguinal hernias in men can be monitored for years per clinical trials, but regular check-ups are essential.
What are the signs a hernia has become an emergency?
Sudden severe pain, irreducible bulge that turns red/purple, vomiting, or inability to pass gas/stool. Go to ER immediately—these indicate possible strangulation.
Is hernia surgery safe and effective?
Yes—modern techniques have low complication rates (<5% major issues) and high success. Mesh repair is standard and well-tolerated.
Can diet, exercise, or natural remedies heal a hernia?
No natural remedy closes the defect. Lifestyle changes help manage symptoms and slow progression but cannot replace surgery when needed.
Do all hernias eventually require surgery?
Not necessarily—some hiatal or small inguinal cases are managed lifelong without operation if asymptomatic. However, most symptomatic hernias benefit from repair.
What’s the difference for children versus adults?
Children (especially infants with umbilical hernias) often experience spontaneous closure. Adults almost never do.
Final Word A hernia cannot heal itself in adults, but that doesn’t mean panic or immediate surgery for everyone. With accurate information, timely evaluation, and modern minimally invasive options, most people achieve excellent outcomes and return to full, active lives.
If you suspect a hernia, schedule an appointment with a general surgeon or hernia specialist today. Early discussion prevents complications and gives you control over your treatment path.
READ ALSO: Hemorrhoid Bleeding How Much Is Normal? Complete Guide to Symptoms, When to Worry, and Proven Relief Strategies