Experts address chronic venous insufficiency fatal concerns often. This condition affects millions worldwide. Veins in legs fail to return blood properly. Blood pools, causing pressure buildup. Symptoms start mild but progress over time. Untreated cases lead to serious issues. Many question chronic venous insufficiency fatal outcomes. Research shows it’s not directly deadly. Complications can threaten life though. Early detection saves lives. Lifestyle changes help manage it. Medical treatments improve blood flow. Prevention reduces risk factors. Understanding CVI empowers patients. Doctors recommend regular checkups. Awareness spreads through education.
Chronic venous insufficiency impacts daily activities. Swelling hinders mobility. Pain disrupts sleep. Skin changes cause embarrassment. Varicose veins appear unsightly. Ulcers form in advanced stages. Infections complicate healing. Blood clots pose dangers. Pulmonary embolism risks rise. Heart strain increases. Quality of life drops sharply. Work productivity suffers. Emotional stress builds up. Family dynamics change. Healthcare costs escalate. Insurance covers some treatments. Support groups offer help. Online resources educate further. Professional advice guides decisions.
Understanding Chronic Venous Insufficiency
Damaged leg veins cause chronic venous insufficiency. Valves malfunction, allowing backward flow. Gravity worsens blood pooling. Deep, superficial, or perforator veins suffer. Post-thrombotic syndrome links to DVT. Scar tissue harms valves post-clot. Congenital issues include missing valves. Primary causes involve vein widening. Secondary factors stem from damage. DVT history heightens risk significantly. Pregnancy strains veins temporarily. Obesity adds extra pressure. Smoking damages vessel walls. Inactivity weakens muscle pumps. Age over 50 increases prevalence. Females face higher odds. Family history plays a role. May-Thurner syndrome compresses veins.
CVI affects one in 20 adults. Varicose veins precede it often. One in three adults has venous disease. Annual progression rate hits one in 50. Legs feel heavy constantly. Tingling sensations occur frequently. Burning pains strike unexpectedly. Cramping disrupts nights. Skin turns reddish-brown. Edema swells ankles post-standing. Itching irritates daily. Leathery texture develops slowly. Ulcers open near ankles. Infections spread if ignored. Scar tissue hardens calves. Mobility decreases over years. Quality of life erodes. Interventions halt advancement. Monitoring tracks changes.
Causes of Chronic Venous Insufficiency
Valve failure triggers CVI primarily. Blood refluxes downward due to gravity. DVT scars veins permanently. Clots damage valve function. Congenital malformations exist from birth. Veins stretch abnormally in primary cases. Injuries harm vein structures. Surgeries sometimes cause complications. High leg pressure builds from standing. Sitting prolongs blood stasis. Phlebitis inflames superficial veins. Hypertension stresses vascular system. Obesity overloads lower extremities. Smoking constricts blood vessels. Lack of exercise weakens calves. Pregnancy hormones relax veins. Hormonal changes affect women more. Genetic factors predispose individuals.
Trauma disrupts normal flow. Blood clots form easily. Inflammation weakens vein walls. Infections exacerbate damage. Tumors rarely block veins. Malignancy develops in ulcers seldom. Aggressive cancers arise occasionally. Chronic conditions compound risks. Diabetes impairs circulation further. Heart failure strains veins. Kidney issues cause fluid retention. Medications influence blood viscosity. Environmental factors play minor roles. Occupational hazards include prolonged postures. Travel restricts movement. Heat dilates veins temporarily.
Symptoms of Chronic Venous Insufficiency
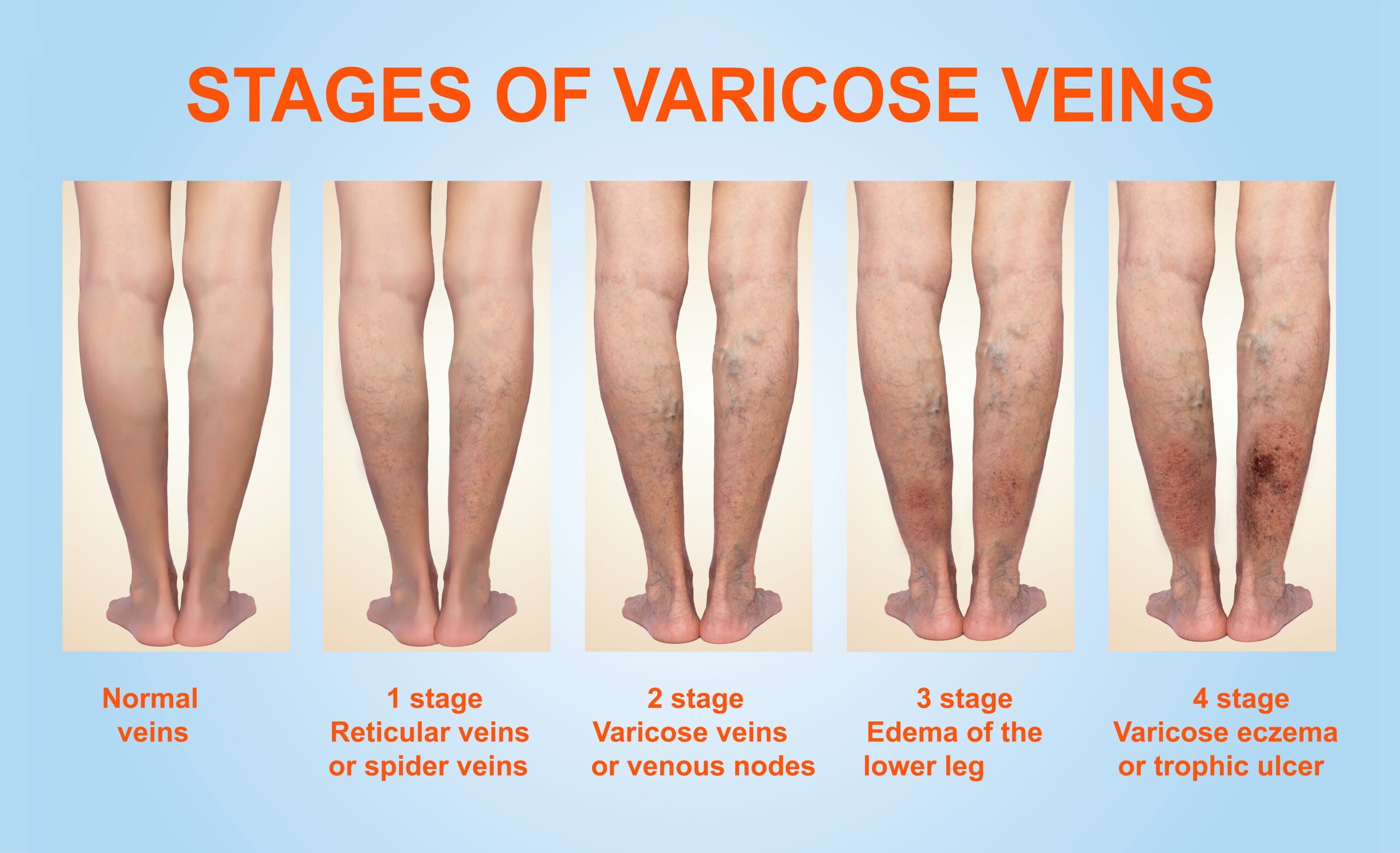
Legs ache after minimal activity. Tiredness sets in quickly. Burning sensations radiate upward. Tingling mimics pins and needles. Cramping strikes at night. Skin discolors to reddish-brown. Swelling inflames lower legs. Ankles puff up post-standing. Flaking skin appears dry. Itching demands scratching. Heaviness weighs down limbs. Leathery skin hardens gradually. Open sores form ulcers. Pain intensifies with infection. Varicose veins bulge visibly. Restless legs urge movement. Charley horses spasm painfully. Tight calves signal issues. Brown spots mark ankles. Walking worsens discomfort.
Symptoms mimic other conditions. Diagnosis requires professional evaluation. Progression varies among patients. Early signs include mild swelling. Advanced stages show ulcers. Infections cause fever sometimes. Mobility limits daily tasks. Sleep disturbances occur frequently. Emotional toll includes depression. Social withdrawal happens often. Work absences increase. Healthcare visits multiply. Medication relieves temporarily. Compression aids symptom control. Elevation reduces edema fast. Exercise improves circulation. Diet influences overall health.
Here are visual examples of CVI symptoms:

:max_bytes(150000):strip_icc()/venuous-insufficiency-overview-4177929-v1-5c3b9644c9e77c0001c7fd3a.png)
Risk Factors for Developing CVI
History of DVT tops risk list. Varicose veins signal early warning. Family genetics heighten susceptibility. Obesity burdens leg veins. Pregnancy multiplies vein pressure. Inactivity stalls blood flow. Smoking harms endothelial lining. Prolonged standing strains valves. Sitting jobs restrict circulation. Chair sleeping pools blood. May-Thurner compresses iliac vein. Female gender increases odds. Age over 50 accelerates onset. Overweight status adds weight. Leg injuries damage vessels. Blood clots recur often. High blood pressure affects veins. Lack of movement weakens pumps. Tobacco use constricts flow.
Risks compound with multiple factors. Women face hormonal influences. Men experience occupational hazards. Elderly lose vein elasticity. Obese individuals carry excess load. Pregnant women gain fluid. Smokers inhale toxins daily. Inactive lifestyles dominate modern society. Standing professions include teachers. Sitting roles encompass office workers. Genetic testing identifies predispositions. Lifestyle assessments reveal habits. Medical history uncovers past events. Preventive measures target risks. Education informs at-risk groups.
Is Chronic Venous Insufficiency Fatal?
Patients worry about chronic venous insufficiency fatal possibilities. Studies link CVI to higher mortality. Direct fatality remains low though. Complications drive death risks. Untreated cases progress dangerously. Blood clots form in veins. Pulmonary embolisms block lungs. Infections spread systemically. Cellulitis requires urgent care. Secondary lymphedema swells tissues. Cardiovascular diseases associate strongly. All-cause death rises 46 percent. Independent of age and sex. Risk factors amplify threats. Comorbidities worsen prognosis. Early treatment prevents fatalities. Monitoring detects complications early.
Chronic venous insufficiency fatal myths persist online. Reality shows manageable condition. Progression causes debility not death. Ulcers lead to amputations rarely. Infections turn septic occasionally. Clots travel to lungs. Embolisms cause sudden deaths. Heart strain from pooling. Reduced mobility invites pneumonia. Depression affects health behaviors. Neglect exacerbates issues. Professional care averts crises. Statistics reveal low direct deaths. 62 U.S. deaths listed CVI. Associations with CVD increase risks. Awareness combats fatal outcomes.
Addressing chronic venous insufficiency fatal concerns matters. Research confirms elevated death risk. Population studies show 40.8 percent prevalence. Higher CEAP classes predict CVD. Follow-up data tracks mortality. Hazard ratios indicate 1.46 increase. Validation in cohorts strengthens evidence. Cardiovascular profiles influence outcomes. Medication adjusts risks minimally. Independent predictors include CVI. Public health implications arise. Screening programs target populations. Interventions lower death rates. Education dispels fatal fears.
Complications Arising from CVI
Untreated CVI bursts capillaries. Tissue inflammation follows quickly. Damage accumulates over time. Venous stasis ulcers form. Healing proves difficult. Infections invade open sores. Cellulitis spreads if ignored. Scar tissue hardens skin. Ulcers recur frequently. Deep vein thrombosis develops. Clots dislodge dangerously. Pulmonary embolism threatens life. Lymphedema damages lymphatics. Swelling persists chronically. Lipodermatosclerosis stiffens legs. Malignancy arises rarely. Aggressive tumors grow fast. Hemorrhage occurs severely. Morbidity rises with progression.
Complications impair daily living. Pain limits activities. Mobility decreases sharply. Infections require antibiotics. Clots demand anticoagulants. Ulcers need dressings. Surgery addresses severe cases. Amputations happen exceptionally. Quality of life suffers. Work capacity drops. Healthcare utilization increases. Costs burden families. Support systems help cope. Research seeks better treatments. Prevention avoids complications. Early signs prompt action.
People fear chronic venous insufficiency fatal complications. DVT leads to embolisms. Ulcers infect deeply. Sepsis endangers organs. Heart failure links indirectly. Stroke risks rise slightly. Kidney strain from fluid. Liver issues emerge rarely. Neurological symptoms appear. Immune system weakens. Overall health declines. Timely care prevents escalation. Specialists manage risks effectively.
Diagnosis of Chronic Venous Insufficiency
Doctors examine legs physically. Swelling indicates issues. Ulcers suggest advanced stage. Skin changes reveal progression. Vascular ultrasound images veins. Sound waves detect damage. Blood flow direction shows reflux. Valve function assesses clearly. MRI rules out mimics. PAD screening accompanies often. Ankle-brachial index measures pressure. History reviews past clots. Symptoms guide questioning. Family background uncovers genetics. Risk factors evaluate thoroughly. Duplex ultrasound confirms structure.
Diagnosis uses non-invasive tests. Ultrasound lasts minutes. Results appear immediately. Specialists interpret findings. Biopsies occur rarely. Blood tests check clotting. Imaging excludes tumors. Consultation involves vascular experts. Early diagnosis improves outcomes. Misdiagnosis delays treatment. Awareness aids accurate detection. Technology advances diagnostics.
Treatment Options for CVI
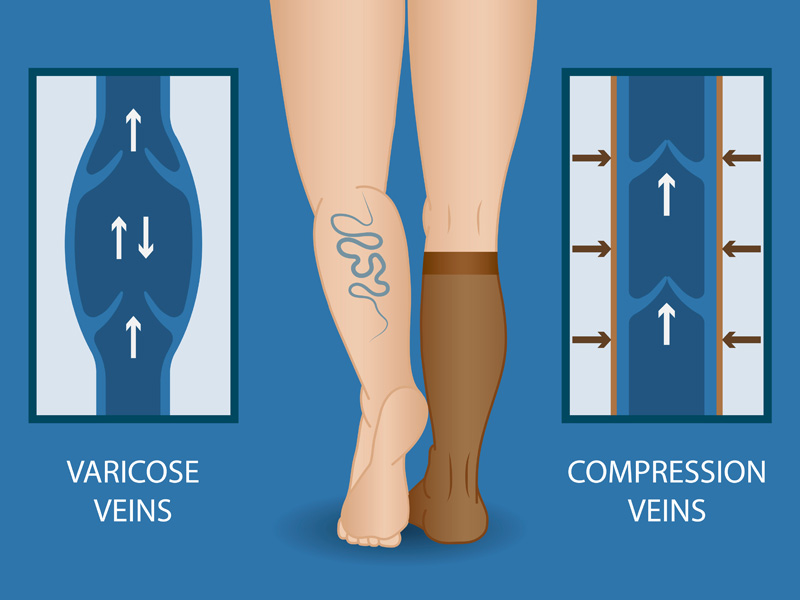
Lifestyle changes start management. Legs elevate above heart. Sessions last 30 minutes. Thrice daily reduces swelling. Walking activates calf pumps. Weight loss eases pressure. Compression stockings squeeze veins. Graduated types tighten ankles. Prescription ensures proper fit. IPC devices pump intermittently. Antibiotics treat infections. Anticoagulants prevent clots. Unna boots wrap medicated. Sclerotherapy injects solutions. Veins collapse permanently. Ablation uses heat energy. Lasers close damaged veins.
Treatments target symptoms effectively. Radiofrequency seals veins. Phlebectomy removes small segments. Ligation ties off vessels. Stripping extracts long veins. SEPS blocks perforators. Bypass reroutes blood flow. Aspirin heals ulcers. Diuretics manage fluid rarely. Endovenous methods minimize invasion. Recovery happens quickly. Outpatient procedures dominate. Follow-up monitors progress. Combinations optimize results. Personalized plans suit patients.
Visualize compression therapy:
Prevention Strategies Against CVI
Avoid smoking to protect vessels. Loose clothing prevents constriction. Movement breaks prolonged postures. Diet limits sodium intake. Exercise strengthens legs. Weight control reduces load. Anticoagulants follow DVT. Stockings compress preventively. Elevation aids daily flow. Activity promotes circulation. Healthy habits build resilience. Genetic counseling informs risks. Occupational changes minimize standing. Travel uses compression gear. Heat avoidance prevents dilation.
Prevention focuses on modifiable factors. Education targets high-risk groups. Screenings detect early. Lifestyle coaching supports changes. Community programs encourage activity. Workplace policies allow breaks. Family support reinforces habits. Long-term adherence prevents onset. Monitoring tracks effectiveness.
Living with Chronic Venous Insufficiency
Patients adapt daily routines. Elevation becomes habit. Compression wears consistently. Exercise integrates smoothly. Diet adjusts healthily. Medication adheres strictly. Checkups schedule regularly. Symptoms monitor closely. Support networks connect peers. Emotional care addresses stress. Work accommodations ease burdens. Travel plans include precautions. Family education fosters understanding. Quality life maintains possible. Positive mindset aids coping. Resources provide guidance.
Living involves ongoing management. Pain relief uses techniques. Mobility aids assist walking. Skin care prevents ulcers. Infection vigilance saves complications. Nutrition boosts healing. Sleep positions elevate legs. Social activities continue adapted. Career choices consider health. Financial planning covers costs. Insurance navigates treatments. Research participation advances knowledge. Advocacy raises awareness.
Concerns about chronic venous insufficiency fatal aspects persist. Management mitigates risks effectively. Education empowers informed choices. Specialists guide long-term care. Technology improves monitoring. Future treatments promise better outcomes.
READ ALSO: Understanding Varicocele Surgery and Its Impact