Pleuropericardial effusion develops when fluid builds up in both pleural and pericardial spaces. This condition impacts lung expansion and heart function. Doctors identify it in patients with underlying systemic issues. Early detection prevents severe complications.
What Is Pleuropericardial Effusion?
Pleuropericardial effusion involves excess fluid around the lungs and heart simultaneously. The pleural space surrounds the lungs. The pericardial sac encases the heart. Fluid accumulation compresses both organs. Patients experience breathing difficulty and cardiac strain. This combined effusion signals serious health problems. Doctors use imaging to confirm fluid in both areas.

The pleural effusion compresses lung tissue. The pericardial effusion restricts heart movement. Together, they reduce oxygen intake and blood circulation. Medical experts classify it as concurrent effusions. This term appears in case reports and reviews.
Causes of Pleuropericardial Effusion
Infections trigger pleuropericardial effusion frequently. Viral infections attack both spaces. Bacterial causes include tuberculosis. Fungal infections occur in immunocompromised patients. Parasitic diseases spread fluid buildup.
Autoimmune disorders cause inflammation. Lupus leads to serositis. Rheumatoid arthritis inflames membranes. Polymyalgia rheumatica presents rarely with this effusion. Connective tissue diseases promote fluid leakage. Neoplastic conditions contribute significantly. Lung cancer metastasizes to pleura. Breast cancer spreads to pericardium. Lymphoma affects both cavities. Malignancies produce exudative fluid.
Heart-related issues generate transudative effusions. Congestive heart failure raises pressure. Cirrhosis impairs fluid balance. Kidney failure causes retention. Iatrogenic factors include drugs. Certain medications induce inflammation. Radiation therapy damages tissues. Procedures cause trauma. Rare causes surprise clinicians. Obstructive uropathy leads to simultaneous effusions. One case report highlighted this mechanism. Idiopathic cases occur occasionally.

Common causes link to systemic illness. Infections dominate in developing regions. Autoimmune diseases prevail in others. Cancer increases with age.
Symptoms and Clinical Presentation
Patients feel shortness of breath. Dyspnea worsens with activity. Orthopnea forces upright position. Chest pain occurs often. Pain sharpens during breathing or coughing. Fatigue drains energy quickly. Palpitations signal heart strain. Dizziness arises from low output. Fainting indicates severe compression.
Cough develops dry or productive. Swelling appears in legs. Hoarseness results from nerve pressure. Hiccups persist in some cases. Mild effusions remain asymptomatic. Rapid buildup causes emergencies. Cardiac tamponade threatens life. Tamponade compresses heart chambers.
Symptoms overlap with individual effusions. Combined presentation heightens severity. Doctors assess vital signs carefully.
Diagnosis of Pleuropericardial Effusion
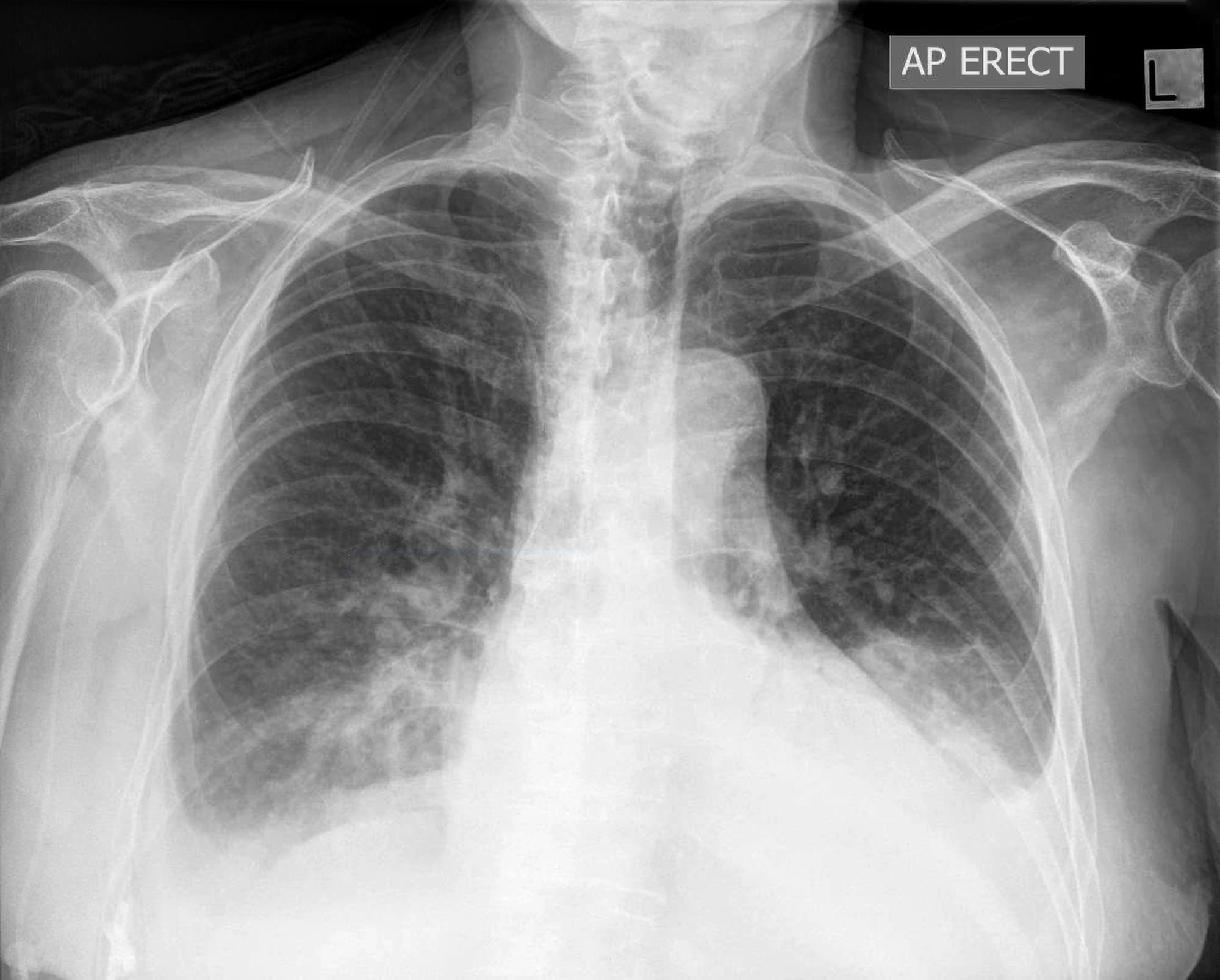
Doctors start with physical examination. They listen for reduced breath sounds. Heart sounds muffle in pericardial cases. Neck veins distend. Chest X-ray reveals fluid levels. Blunting of costophrenic angles indicates pleural fluid. Enlarged cardiac silhouette suggests pericardial involvement.
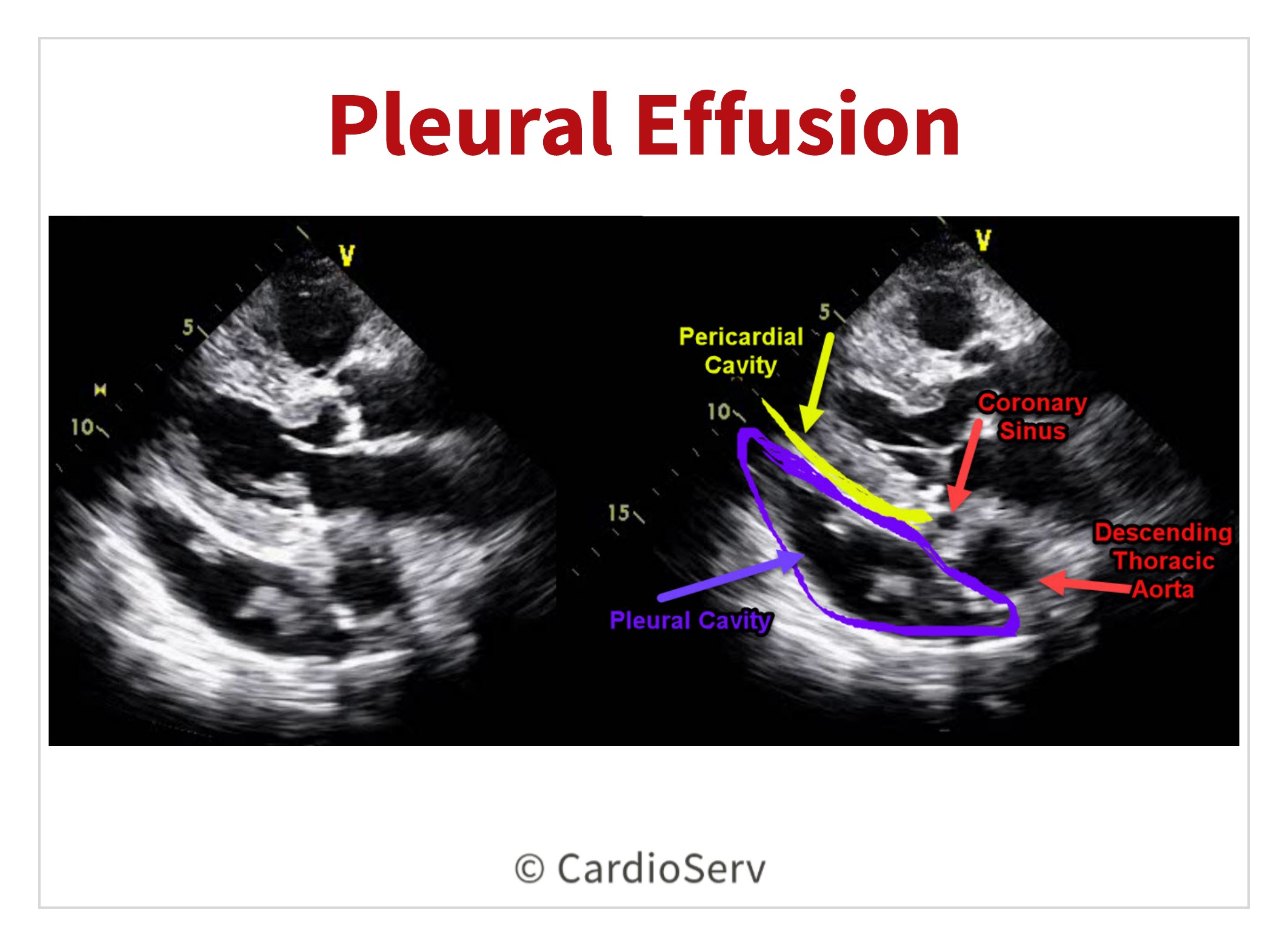
Ultrasound detects effusions quickly. Echocardiogram visualizes pericardial fluid. It assesses tamponade signs. CT scan provides detailed images. It differentiates causes. MRI offers soft tissue contrast.
Thoracentesis samples pleural fluid. Pericardiocentesis drains pericardial fluid. Analysis checks protein, cells, and cultures. Blood tests identify inflammation. Elevated ESR signals autoimmune issues. Tumor markers screen malignancies.
Doctors integrate findings. They rule out common causes first. Rare etiologies require deeper investigation.
Treatment Approaches for Pleuropericardial Effusion
Treatment targets the underlying cause. Doctors prescribe antibiotics for infections. Antivirals combat viral origins. Anti-inflammatory drugs reduce autoimmune inflammation. Corticosteroids relieve symptoms quickly. Immunosuppressants manage chronic cases.
Diuretics remove excess fluid. They help heart failure patients. Chemotherapy treats malignant effusions. Drainage procedures relieve pressure. Thoracentesis removes pleural fluid. Pericardiocentesis drains pericardial space. Catheters stay for recurrent cases.
Surgery creates windows. Pericardial window drains into pleural space. Pleurodesis prevents recurrence. VATS minimizes invasiveness. Supportive care stabilizes patients. Oxygen therapy aids breathing. Pain management improves comfort. Monitoring prevents complications. Serial imaging tracks progress. Fluid reaccumulation requires intervention.

Multidisciplinary teams collaborate. Pulmonologists handle pleural issues. Cardiologists manage pericardial aspects. Oncologists address cancers.
Complications and Prognosis
Untreated pleuropericardial effusion leads to tamponade. Cardiac output drops sharply. Shock develops rapidly. Respiratory failure occurs from lung compression. Hypoxemia worsens organ function. Empyema complicates infected effusions. Prognosis depends on cause. Infectious cases respond well to treatment. Autoimmune conditions manage chronically.
Malignant effusions carry poorer outlook. Early intervention improves survival. Idiopathic cases resolve spontaneously. Recurrence poses challenges. Pleurodesis reduces risk. Regular follow-up detects issues. Patients recover with prompt care. Lifestyle changes support healing. Smoking cessation aids lung function.
Prevention and Long-Term Management
Prevent underlying diseases. Vaccinate against infections. Control autoimmune flares. Monitor heart and kidney health. Regular check-ups catch early signs. Imaging screens high-risk patients. Blood tests track inflammation. Healthy habits reduce risks. Balanced diet prevents fluid retention. Exercise strengthens cardiovascular system.
Education empowers patients. They recognize warning symptoms. Prompt reporting improves outcomes. Research advances understanding. New therapies target causes. Improved drainage techniques enhance safety. Pleuropericardial effusion demands attention. Doctors act swiftly. Patients follow treatment plans. This approach restores health effectively.
READ ALSO: The Vital Role of Histology Technicians in Healthcare